
For decades, surgeons relied on 2D X-rays and tactile intuition to position an implant during hip replacement surgery. However, the introduction of the direct anterior approach has shifted the focus toward extreme precision and muscle preservation. Explore how specialists can now utilize 3D imaging to map every millimeter of a patient's anatomy and virtually plan the surgery before ever entering the operating room.
Why CT Scans Provide Better Planning for Hip Replacement Surgery
Traditional preoperative planning relies on two-dimensional X-rays, which can be misleading. A 2D image cannot account for the unique "rotation" of a patient's pelvis or the specific depth of their hip socket.
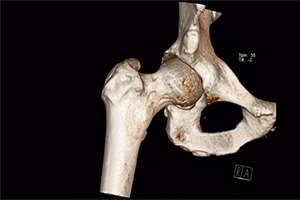
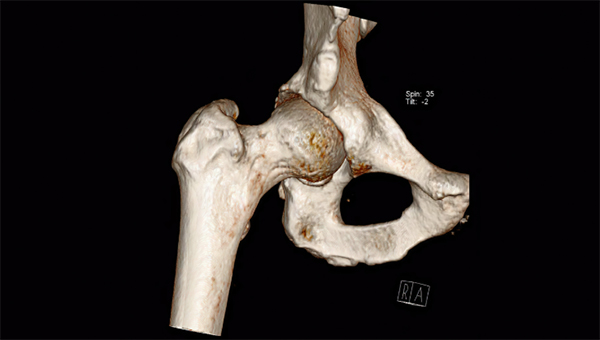
By contrast, a CT scan provides a high-resolution, 3D digital blueprint of the bone. This allows the surgeon to see the exact thickness of the pelvic wall and the true shape of the femoral canal. When we know the exact topography of the bone, we can select the perfect implant size and orientation, reducing the risk of a "mismatch" that could lead to discomfort or early wear.
The Power of Mako SmartRobotics™ Integration
One of the most significant reasons for the shift toward CT-based planning is the integration of the Mako robotic-arm system. Unlike other surgical guides that rely on general estimates, the Mako system uses the patient’s specific CT data to create a personalized virtual model.
During a direct anterior hip replacement, the robot provides real-time haptic feedback. This means the surgeon can only remove the bone specified in the 3D plan. This virtual boundary protects healthy bone and ensures the cup is placed at the optimal angle to prevent dislocation. The Mako system essentially transforms the surgeon’s qualitative judgment into quantitative data, ensuring the implant fits the patient's unique anatomy like a key in a lock.
Improving Hip Stability and Balance with CT-Guided Planning
Two of the most common concerns for hip replacement patients are leg length discrepancy and a "natural" feeling joint. CT-based planning is the gold standard for solving these issues.
Because the 3D model includes the entire pelvis and the relationship between both hips, the surgeon can calculate the exact offset (the distance the femur sits from the pelvis) and leg length. This level of detail is nearly impossible to achieve with 2D templating alone. For the patient, this means a more balanced gait and a joint that feels stable from the very first step.
A "Reset" for Your Natural Hip Biomechanics
Ultimately, CT-based planning is about more than just technology; it is about restoring the natural harmony of your body. By combining the muscle-sparing benefits of the direct anterior approach with the data-driven precision of a 3D plan, we can significantly increase the longevity and comfort of your new hip.
Frequently Asked Questions
- Why do surgeons use CT scans before hip replacement surgery?
CT scans provide a detailed 3D view of the hip joint, allowing surgeons to precisely evaluate bone shape, alignment, and implant positioning. This level of detail helps improve surgical accuracy and reduces the risk of implant mismatch compared to traditional X-ray planning.
- What is Direct Anterior Hip Replacement?
Direct anterior hip replacement is a minimally invasive technique that allows the surgeon to access the hip joint from the front of the body. This muscle-sparing approach may lead to faster recovery, less post-operative pain, and improved early mobility for many patients.
- Can CT-based planning help prevent leg length differences after hip replacement?
Yes. CT-guided planning allows surgeons to measure the relationship between the pelvis and femur with high accuracy. This helps restore proper leg length and hip offset, improving balance, walking mechanics, and overall joint stability.
- Does CT-based planning improve long-term hip replacement outcomes?
Precise implant positioning and better alignment can reduce wear on the artificial joint and improve stability. By combining CT-based planning with modern surgical techniques, surgeons aim to create a hip replacement that functions more naturally and lasts longer.
Reference Links:
AUTHOR: Nathan Odor, M.D. – Orthopedic Hip & Knee Surgeon
Nathan Odor, M.D. is a board-certified and fellowship-trained orthopedic surgeon at the Oklahoma Joint Reconstructive Institute, specializing in hip and knee replacement, including complex primary and revision procedures. Dr. Odor is committed to helping patients regain mobility, reduce pain, and improve quality of life through personalized, patient-centered care across Oklahoma.
Credentials & Recognition
Dr. Odor earned his medical degree from the University of Oklahoma College of Medicine, where he also completed his residency in orthopedic surgery. He completed a fellowship at the Colorado Orthopaedic Research Institute focused on advanced hip and knee reconstruction. Dr. Odor is board-certified and fellowship-trained, with specialized expertise in robotic-assisted surgery and the direct anterior approach for hip replacement.
Clinical Expertise
Dr. Odor is a member of the American Academy of Orthopaedic Surgeons (AAOS) and specializes in minimally invasive hip and knee replacement, robotic-assisted joint surgery, and personalized recovery protocols. He emphasizes patient education, compassionate care, and innovative surgical techniques to enable faster recovery and optimal long-term outcomes. His approach integrates advanced technology with evidence-based pain management to support safer, more efficient rehabilitation.
Medical Disclaimer: This information is for educational purposes only and does not constitute medical advice. For diagnosis and treatment recommendations, please consult with Dr. Nathan Odor or another qualified orthopedic specialist.
Content authored by Dr. Nathan Odor, M.D., and verified against official sources.

